What is Tinnitus?
Tinnitus comes from the Latin word “tinnire” which means “to ring”. It is defined as any sound perceived by the patient when no external source exists. It is described by the patient as ringing, buzzing or whistling sound heard either in one ear or both the ears. It is a condition that impinges on the life sufferers to varying degrees. Insomnia, inability to concentrate and depression are commonly reported to accompany the condition.
How common is tinnitus?
As many as one third (32%) of Americans experience tinnitus sometime in their lives. It is estimated that approximately 18 million Americans seek medical attention for this symptom. Nine million reported to be seriously affected by this condition and 2 million are disabled because of this elusive sound. Patients who suffer from this chronic symptom report a dwindling in their quality of life, primarily because of the annoyance factor associated with it. Activities of daily living are affected in proportion to the intensity of tinnitus.
How do you classify a patients’ tinnitus?
It is classified into two categories- subjective and objective. Objective Tinnitus is infrequent and is audible to the examiner. Subjective Tinnitus is much more common and is not audible to the examiner.
What are the causes of tinnitus?
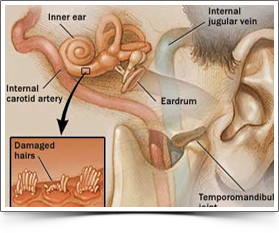
 Subjective Tinnitus- generally associated with hearing loss as a result of noise exposure or ageing.
Subjective Tinnitus- generally associated with hearing loss as a result of noise exposure or ageing.- Otologic- Impacted wax
- Fluid in the middle ear
- Acute and chronic otitis media
- Abnormally patent eustachian tube
- Meniere’s disease
- Otosclerosis
- Presbyacusis
- Noise trauma
- Ototoxic drugs
- Tumours of nerve of hearing
- Non otologic-Disease of CNS
- Anaemia
- Arteriosclerosis
- Hypertension
- Hypotension
- Hypoglycemia
- Epilepsy
- Migraine
Objective Tinnitus-Vascular disorders may cause pulsatile Tinnitus by generating turbulent flow in blood vessels in neck or temporal bone. These include venous hums, arterial bruits, arteriovenous malformations, aneurysms, aberrant vessels and vascular neoplasm. Neurological disorder includes palatal myoclonus and stapedius and tensor tympani muscle spasm (middle ear muscle spasm).
Investigation done in patients with tinnitus:
- Otoscopic examination of the ear.
- Pure tone audiometry
- Impedence audiometry
- ENG
- ECG
- BERA
- Blood sugar
- Thyriod function test
- Lipid profile
- Serological test for syphilis
- CT Scan
- MRI
- Angiography
Management of tinnitus
Counseling- Patients has to be helped to understand and learn to cope with Tinnitus. It is the most important single component in management of Tinnitus. Psychological treatment- relaxation training therapy helps to teach patients to learn to relax in the face of stress-full event.
Medical treatment for causative disorders
- Non specific medical treatments are tranquilizers, antidepressants and sedative drugs. Tension and insomnia created by tinnitus sets up a vicous circle with tinnitus. It may then be very helpful to use these drugs to break the circle.
- Anti-Tinnitus drugs- i.v. lignocaine, clonazepan, carbamazepine, amylobarbitone, phenyton sodium, sodium valproate, intra tympanic steroids.
- Hearing aid- If the patient has hearing impairment, they can be benefited by hearing aid. By improving the patient’s hearing, hearing aid lessens the attention patient gives to tinnitus and thus acts as masker.
- Tinnitus maskers- two types of maskers are non wearable or environmental masker (noisy fan, clock, underpillow speaker, television & cassette player), wearable (behind the ear and in the ear maskers).
- Dietary supplements- zinc sulphate, vitamins and ginkobiloba extract.